Cranium Dysfunctions
1. Flexion.
2. Extension.
3. Torsion.
4. Lateral Flexion-Rotation (Lat.Flex.Rot.)
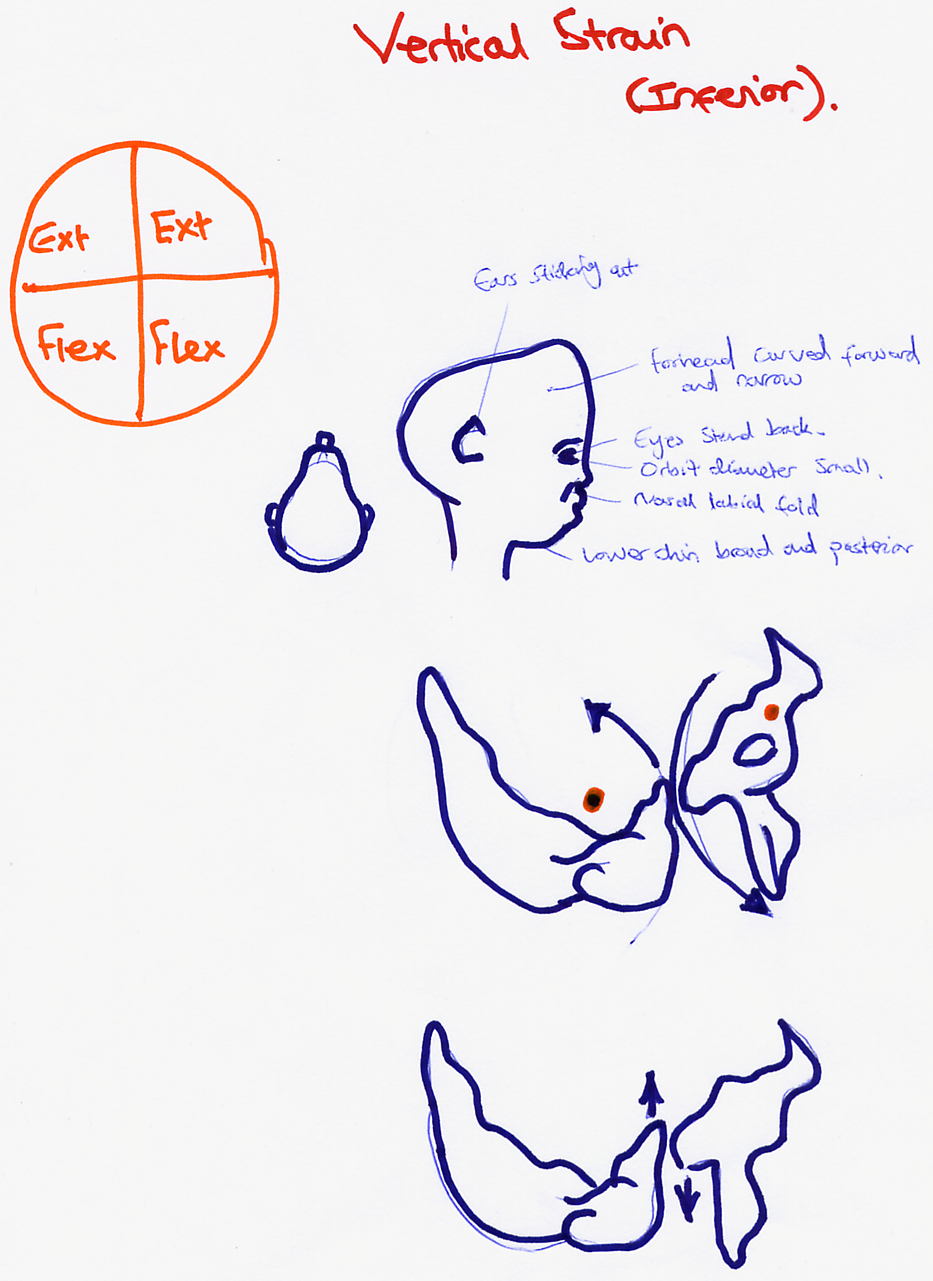
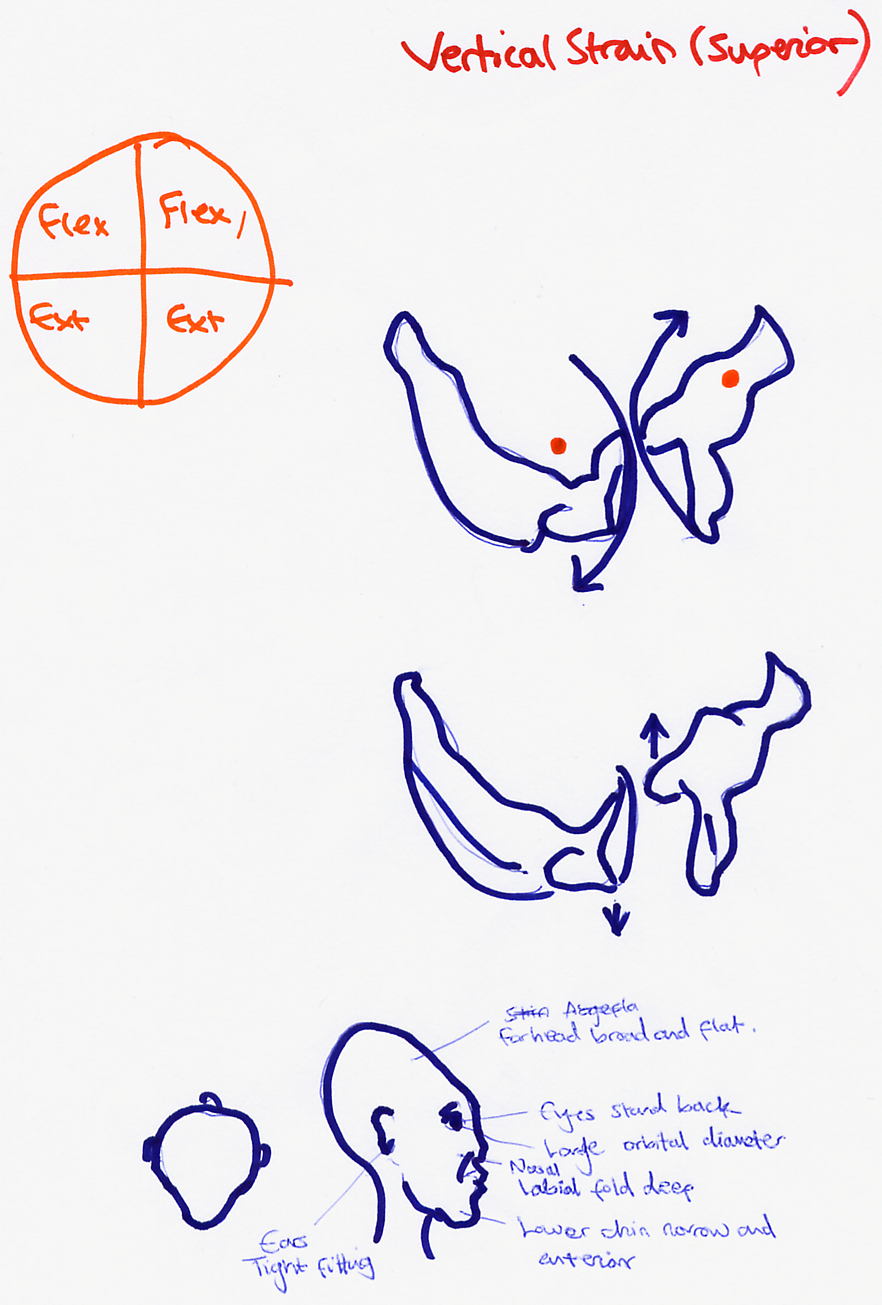
5. Superior and Inferior Vertical Strain.
6. Compression.
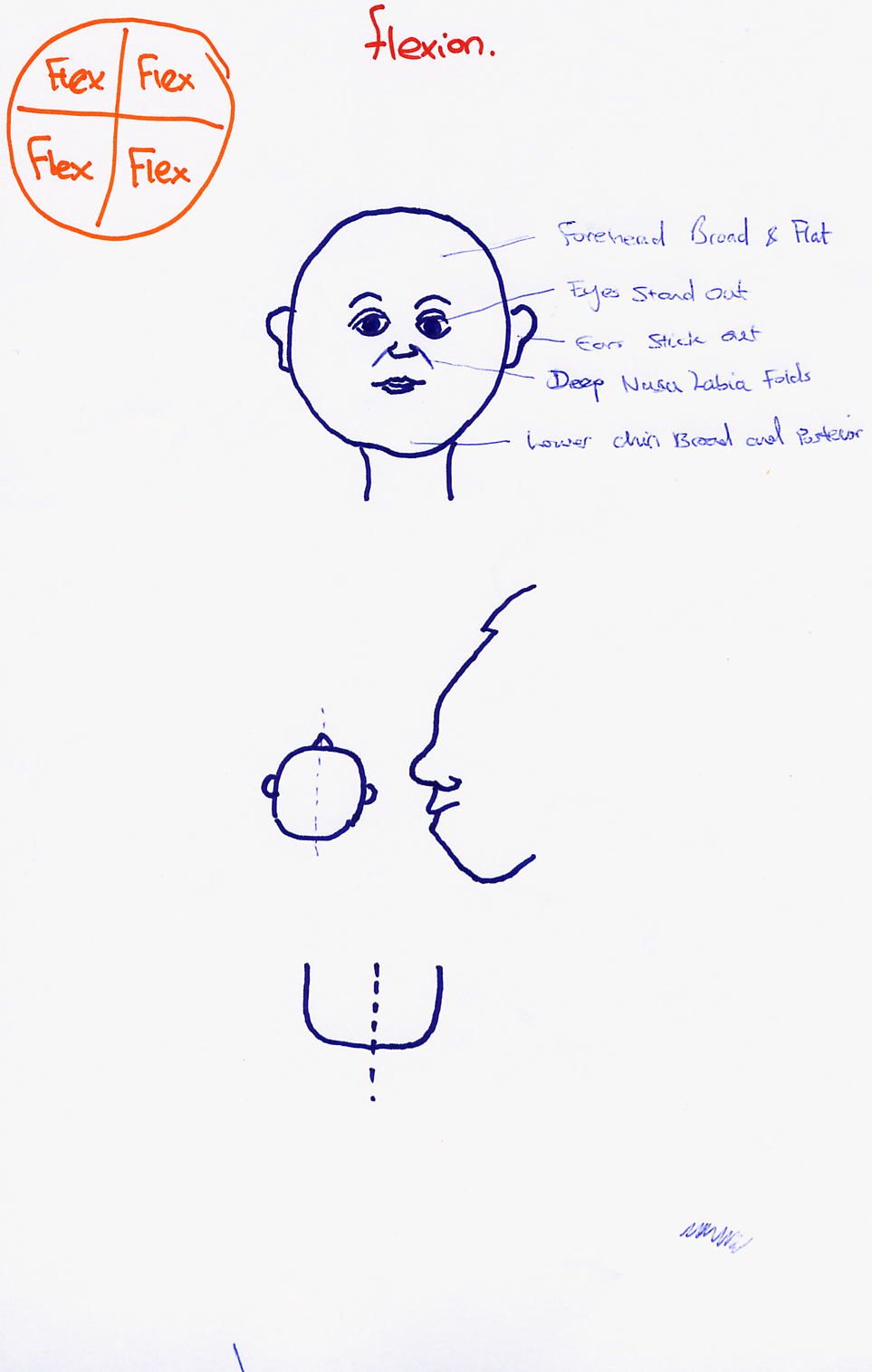
Flexion Dysfunction
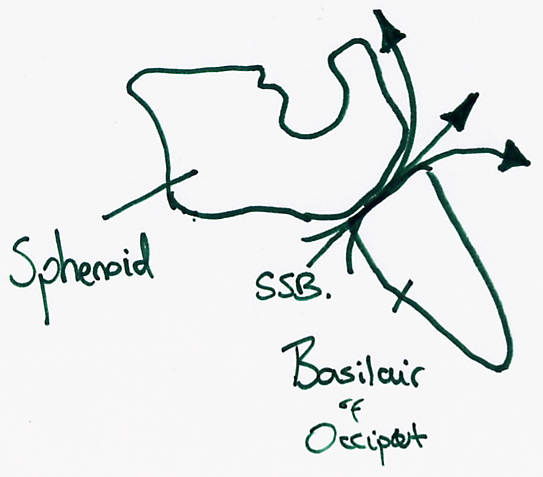
- The axes of movement: Two transversal axes. One axis running through the Sphenoidal Greater Wing, anterior to the Sella Turcica, and the other through the upper-back , upper-half section of the foramen magnum, with respect to the processus jugularis.
- The Sphenoid bone moves more easily and with a greater amplitude in flexion than in extension i.e. the back part of the body of the Sphenoid moves superior. The front part of the Pars Basilaris of the Occiput moves easily superior.
Diagnostic Points
- The Greater Sphenoidal Wings move easily anterior, inferior and lateral.
- The Transversal diameter of the skull becomes larger.
- The forehead is flattened and broad.
- The lateral edges of the processus zygomatici of the Frontal bone are shifted forwards.
- The eyes stand forward, where the anterior-posterior diameter of the orbita becomes smaller.
- The slope diameter of the orbitar become larger (from superior medial to posterior lateral).
- The Nasolaialfalti are deep because of the outward rotation of the upper Sphenoid.
- The roof of the palette is even, broad and shifted posteriorly.
- The horizontal parts of the Mandibula are broadened and shifted posterior, where the temporal bones are in outer-rotation and the Fossae Mandibulares are found in posterior-medial.
- The lateral corner of the temporal line is moved infeior-lateral.
- The Squama Occipitalis is angled.
- The ears stand out, where the temporal bone is in outer-rotation.
- The whole skull is in outer-rotation.
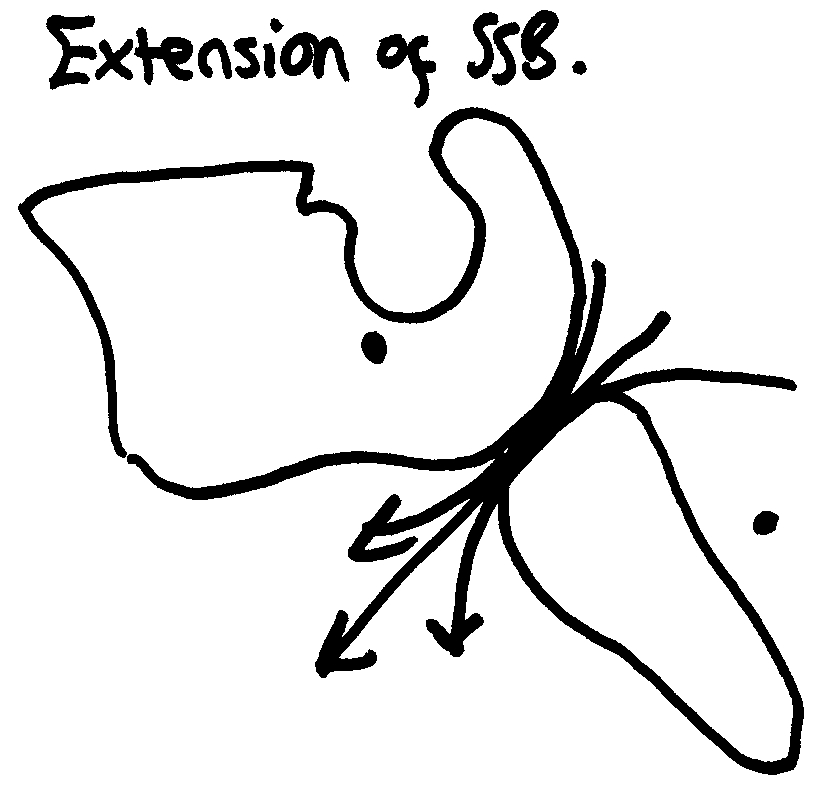
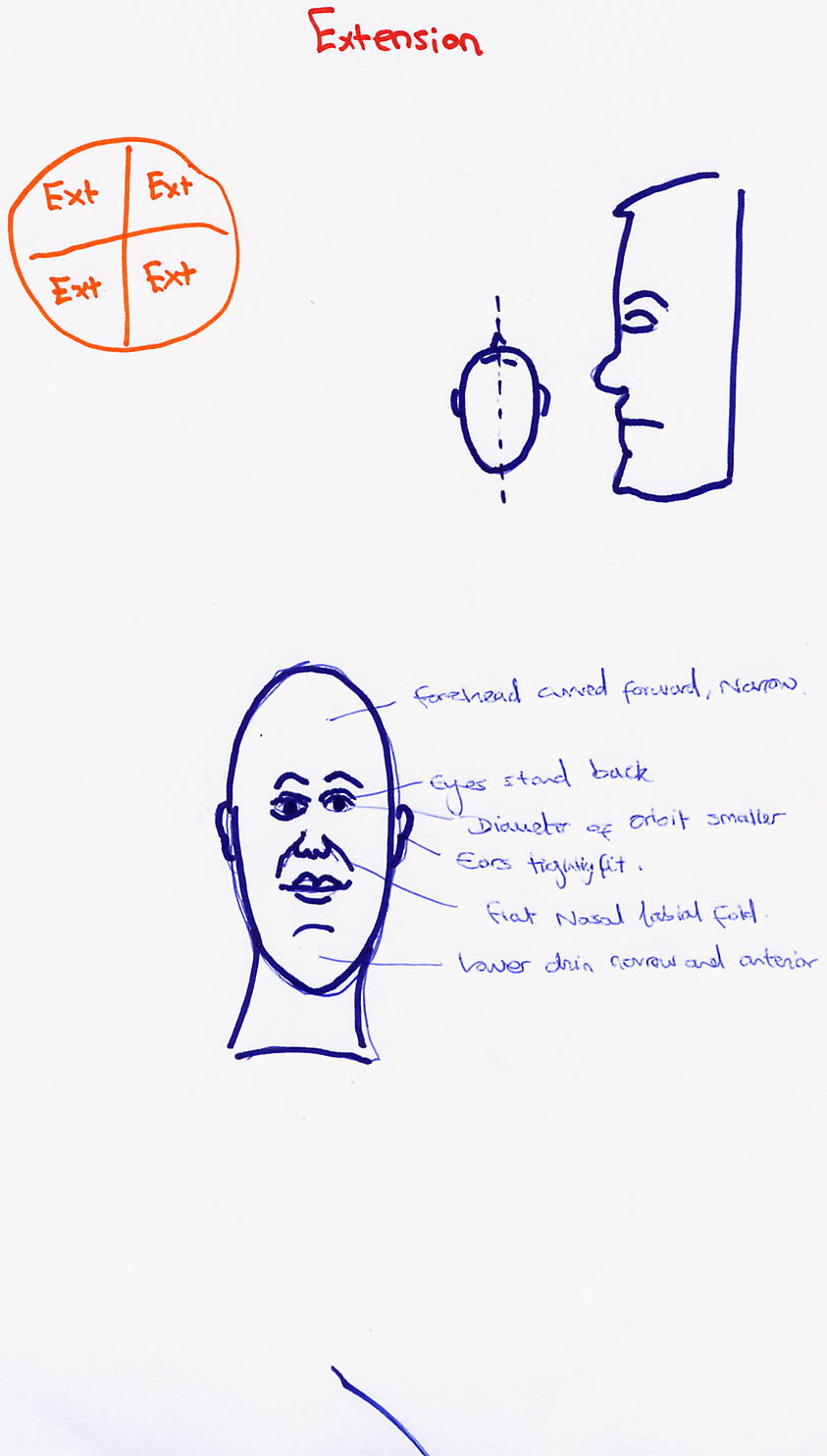
Extension Dysfunction

Lateral Strain